
Research progress of internal limiting membrane dissection for idiopathic macular hole
-
摘要:
玻璃体切除联合内界膜(ILM)剥离是特发性黄斑裂孔(IMH)的有效治疗方法。IMH的预后与裂孔大小及病程长短密切相关。直径 < 400 μm的裂孔有自发闭合的可能, >400 μm的裂孔很少能够自行闭合, 需要玻璃体切除联合ILM剥离解除玻璃体黄斑牵引,才能达到理想的裂孔闭合率。部分直径>400 μm、病程长(6~12个月)的IMH, 单纯ILM剥除效果欠佳,常在ILM剥离的基础上联合应用气体填充、孔周按摩、自体血填充等手术方式优化治疗效果。但是,有研究者认为ILM剥离会造成视网膜显微结构及视功能损害。近些年ILM剥离技术不断改进,衍生出保留中心凹ILM剥离、向心牵引ILM剥离、根据黄斑裂孔(MH)形状定制ILM剥离、各种类型的ILM瓣等技术,以及ILM磨损、奥克纤溶酶药物治疗等其他方法,在保证治疗效果的基础上尽可能降低对视网膜的损害。本文基于国内外学者的临床经验,对ILM剥离治疗IMH最新进展进行综述,明确不同治疗和手术方式的特点和适用性,为临床上IMH的治疗提供参考。
Abstract:Vitrectomy combined with internal limiting membrane (ILM) dissection is an effective therapeutic method for idiopathic macular hole (IMH). The prognosis of IMH is closely related to size of hole and course of disease. The hole with a diameter < 400 μm may close spontaneously, while MH with a diameter >400 μm can rarely close spontaneously, and vitrectomy combined with ILM dissection is required to relieve the vitreous fovea traction, so as to achieve the ideal closure rate of macular hole. For some IMH patients with diameter >400 μm and a long course of disease (6 to 12 months), the ILM dissection alone is not well, and often requires to combined with gas filling, massage around macular hole and autologous blood filling to optimize surgery effect. However, some researchers believe that ILM dissection can cause damage to retinal microstructure and visual function. In recent years, the ILM dissection technology has been continuously improving, technologies are derived such as ILM dissection retaining fovea, centripetal traction ILM dissection, customized ILM dissection according to macular hole (MH) shape, various types of ILM flaps, and other methods such as ILM abrasion and ocriplasmin treatment, so as to reduce retinal damage as far as possible on the basis of ensuring the therapeutic effect. This paper reviewed the latest progresses of ILM dissection in the treatment of IMH based on the clinical experience of domestic and foreign scholars, in order to clarify the characteristics and applicability of different treatment and surgical methods, and provide reference for the clinical treatment of IMH.
-
原发性干燥综合征(pSS)是一种自身免疫性疾病,其发病原因尚未明确,可能与免疫、遗传、感染等因素有关[1]。pSS的典型临床表现为口眼干燥、疲劳及疼痛等,并可累及多个系统。pSS患者中有30%~40%伴有全身性并发症,导致预后不良[2]。由于肺部组织中含有丰富的脉管及结缔组织,是pSS较常累及的器官; 研究[3-4]显示,淋巴细胞性间质性肺炎及淋巴瘤是pSS累及肺部的典型病理学特点, 9%~75%的pSS患者会出现肺部受累,常表现为间质性肺疾病(ILD), 而pSS-ILD患者的生活质量明显降低,病死率明显增高。既往有关pSS-ILD影响因素的研究报道尚无确切定论。因此,本研究分析原发pSS-ILD患者的发生率及危险因素,以期为pSS-ILD的早期诊断、干预提供依据,现报告如下。
1. 资料与方法
1.1 一般资料
回顾性纳入2010年6月—2020年12月本院收治的278例pSS患者,按照肺部高分辨CT检查结果分为pSS-ILD组83例与pSS组195例。纳入标准: ⑴患者的pSS诊断符合《原发性干燥综合征2002年国际分类(诊断)标准》[5]。①口干燥症状(3项中有1项或1项以上); ②眼干症状(3项中有1项或1项以上); ③眼部体征(1项或1项以上阳性); ④组织学检查为小唇腺淋巴细胞灶≥1; ⑤唾液腺受损(1项或以上阳性); ⑥自身抗体为抗SSA和/或抗SSB(+)。⑵患者年龄≥18岁。⑶临床及影像学资料完整者。⑷患者及家属均知情同意。排除标准: ①合并其他自身免疫性疾病、结缔组织疾病和其他肺部疾病者; ②伴有肿瘤、感染、肝脏疾病、贫血、肾衰竭等疾病者; ③既往进行过胸部放疗、肺泡灌洗等治疗者; ④已知其他原因(如药物、职业暴露等)导致的ILD者。本研究经过医学伦理审查。
1.2 方法
所有pSS患者均进行了高分辨CT检查,影像学表现为磨玻璃影、蜂窝影、网格影等判定为pSS-ILD, 判定结果由2位呼吸科医师和2位影像科医师共同确定。
1.3 观察指标
收集2组患者的基线资料、临床症状、实验室指标。①基线资料主要包括性别、年龄、病程、吸烟史等; ②临床症状主要包括发热、口干、眼干、关节疼痛、雷诺现象、咳嗽、咳痰、胸闷气喘、乏力等; ③实验室指标主要包括白细胞(WBC)、血红蛋白(Hb)、血小板(PLT)、嗜中性粒细胞、血沉(ESR)、C反应蛋白CRP)、补体C3、补体C4、免疫球蛋白A(IgA)、免疫球蛋白G(IgG)、免疫球蛋白M(IgM)、类风湿因子、抗核抗体滴度、抗SSA抗体、抗SSB抗体等。
1.4 统计学分析
采用SPSS 22.0统计学软件进行数据分析; 符合正态分布的计量资料以(x±s)表示,两两比较采用t检验; 非正态分布的计量资料以[M(P25, P75)]表示,比较采用非参数检验; 计数资料以[n(%)]表示,比较采用χ2检验; 采用多因素Logistic回归分析探讨pSS-IPD的危险因素; P < 0.05为差异有统计学意义。
2. 结果
2.1 2组基线资料比较
经肺部高分辨CT检查, 278例pSS患者中诊断出pSS-ILD患者83例,发生率为29.86%。pSS-ILD组的年龄大于pSS组,吸烟史比例高于pSS组,差异有统计学意义(P < 0.05); 2组性别构成及病程比较,差异均无统计学意义(P>0.05)。见表 1。
表 1 2组基线资料比较(x±s)[n(%)]组别 n 性别 年龄/岁 吸烟史 病程/月 男 女 pSS-ILD组 83 23 60 56.47±4.80* 31(37.35)* 24.29±5.63 pSS组 195 48 147 50.58±2.16 28(14.36) 23.10±4.47 与pSS组比较, *P < 0.05。 2.2 2组临床症状比较
pSS-ILD组的咳嗽、咳痰及胸闷气喘发生率高于pSS组,差异有统计学意义(P < 0.05); 2组之间其他临床症状发生率比较,差异均无统计学意义(P>0.05)。见表 2。
表 2 2组临床症状比较[n(%)]临床症状 pSS-ILD组(n=83) pSS组(n=195) 口干 40(48.20) 98(50.26) 眼干 38(45.78) 84(43.08) 腮腺炎 1(1.20) 3(1.54) 雷诺现象 6(7.23) 7(3.59) 龋齿 3(3.61) 3(1.54) 关节疼痛 29(34.94) 61(31.28) 皮疹 7(8.43) 18(9.23) 咳嗽 64(77.11)* 20(10.26) 咳痰 50(60.24)* 5(2.56) 胸闷气喘 53(63.86)* 15(7.69) 乏力 13(15.67) 33(16.92) 消化系统受累 43(51.81) 85(43.59) 与pSS组比较, *P < 0.05。 2.3 2组实验室指标比较
pSS-ILD组的WBC、嗜中性粒细胞、补体C3、补体C4水平及抗核抗体滴度、抗SSA抗体阳性率高于pSS组,差异有统计学意义(P < 0.05); 2组之间其他实验室指标比较,差异均无统计学意义(P>0.05)。见表 3。
表 3 2组实验室指标比较(x±s)[n(%)][M(P25, P75)]实验室指标 pSS-ILD组(n=83) pSS组(n=195) WBC/(×109/L) 6.78±1.15* 5.24±0.97 Hb/(g/L) 123.50±18.22 121.61±17.25 PLT/(×1012/L) 210.47±23.68 205.66±19.80 嗜中性粒细胞/(×109/L) 5.12±1.09* 3.38±0.47 ESR/(mm/h) 15.70(10.60, 25.35) 13.42(8.86, 22.10) CRP/(mg/L) 2.36(1.04, 9.64) 1.65(0.90, 7.21) 补体C3/(g/L) 1.15(0.84, 1.68)* 0.89(0.70, 1.12) 补体C4/(g/L) 0.37(0.13, 0.59)* 0.18(0.10, 0.33) IgA/(g/L) 2.50(1.12, 3.55) 2.40(1.06, 3.42) IgG/(g/L) 11.32(9.11, 14.69) 12.38(9.30, 14.75) IgM/(g/L) 1.12(0.71, 1.46) 1.05(0.66, 1.38) 类风湿因子/(IU/mL) 12.40(9.17, 38.90) 12.16(8.96, 37.58) 抗核抗体滴度(1∶x) 1 310.58(665.20, 1 576.40)* 627.30(359.11, 975.43) 抗SSA抗体阳性 62(74.70)* 99(50.77) 抗SSB抗体阳性 13(15.66) 25(12.82) WBC: 白细胞; Hb: 血红蛋白; PLT: 血小板; ESR: 血沉; CRP: C反应蛋白; IgA: 免疫球蛋白A; IgG: 免疫球蛋白G;
IgM: 免疫球蛋白M。与pSS组比较, *P < 0.05。2.4 多因素Logistic回归分析
以pSS-ILD组与pSS组之间具有统计学差异的年龄、吸烟史、咳嗽、咳痰及胸闷气喘、WBC、嗜中性粒细胞、补体C3、补体C4、抗核抗体滴度、抗SSA抗体阳性率为变量进行多因素Logistic回归分析,结果显示: 年龄、吸烟史及抗核抗体滴度是pSS患者发生ILD的独立影响因素(P < 0.05)。见表 4。
表 4 pSS-ILD危险因素的多因素Logistic回归分析因素 B SE Wald χ2 P OR 95%CI 年龄 -0.216 0.115 17.482 < 0.001 0.814 0.620~1.147 吸烟史 -0.351 0.247 6.259 0.013 0.712 0.557~0.960 咳嗽 -0.096 0.055 1.136 0.099 0.381 0.133~0.582 咳痰 -0.043 0.072 0.894 0.211 0.447 0.235~0.691 胸闷气喘 -0.075 0.103 0.936 0.105 0.503 0.314~0.744 白细胞计数 -0.104 0.098 1.081 0.094 0.416 0.220~0.657 嗜中性粒细胞 -0.082 0.075 0.715 0.360 0.354 0.170~0.582 补体C3 -0.100 0.108 0.854 0.219 0.490 0.237~0.685 补体C4 -0.74 0.066 0.912 0.101 0.505 0.311~0.720 抗核抗体滴度 -0.418 0.265 5.336 0.021 0.764 0.528~0.995 抗SSA抗体阳性 -0.079 0.058 1.226 0.086 0.437 0.215~0.680 3. 讨论
pSS能够通过淋巴细胞和浆细胞对靶器官进行浸润,对靶器官造成损伤。pSS患者出现肺部受累在临床上比较常见,临床表现多样化,而ILD是最为常见的肺部受累类型。一旦合并ILD, 患者的预后更差,病死率更高, 5年病死率超过15%, 10年病死率增高4倍[6]。因此对pSS-ILD的发生率进行调查,对相关危险因素进行分析,具有重要的临床意义。一项基于853例pSS患者的队列研究[7]发现, 165例pSS患者合并ILD, pSS-ILD的发生率为19.34%; 黄菁梅等[8]研究显示, pSS-ILD的发生率为50%(15/30); 陈晓静等[9]对非吸烟女性pSS-ILD进行了研究,发现pSS-ILD的发生率为41.46%(34/82)。本研究调查显示, pSS-ILD的发生率为29.86%(83/278), 与相关研究存在差异,可能与样本量、样本来源及诊断方式有关。
一项研究[10]发现,与单纯pSS患者比较, pSS-ILD患者的年龄更大,吸烟比例更高; 也有研究[11]显示, pSS-ILD患者的吸烟比例明显高于单纯pSS患者; 但也有研究[12]证实吸烟比例在2组之间无明显差异。本研究中, pSS-ILD患者的年龄大于单纯pSS患者,吸烟史比例明显高于单纯pSS患者,与齐海宇等[13]的研究结果一致; 将年龄、吸烟史纳入多因素Logistic回归分析,结果显示高龄及吸烟是pSS患者发生ILD的独立危险因素,与GAO H等[7]的研究一致,分析原因可能是高龄患者机体中诱发自身免疫功能发生变化的物质更多,从而导致肺间质纤维化,而吸烟是促进肺部纤维化的重要因素。
pSS-ILD患者的临床症状多样,特异性不强。与单纯pSS患者相比, pSS-ILD患者以干咳为主要临床表现,咳嗽、胸闷等上呼吸道症状的发生率为40%~60%[14]。本研究中pSS-ILD患者的咳嗽、咳痰及胸闷气喘发生率明显高于单纯pSS患者,与黄春艳[15]研究结果相符; 但是高鑫等[16]研究表明pSS-ILD患者的口干、眼干、关节肿痛发生率更低,而本研究中2组之间无明显差异,可能与病情程度有关。以往研究[17]证实, pSS患者中的血清抗SSA抗体、抗SSB抗体、抗核抗体、类风湿因子等血清学指标升高与ILD的发生存在着密切关系。本研究中pSS-ILD患者WBC、嗜中性粒细胞、补体C3及补体C4水平,抗核抗体滴度,抗SSA抗体阳性率明显高于单纯pSS患者,与宋国婧等[18]研究结果基本一致; 但多因素Logistic回归分析显示咳嗽、咳痰及胸闷气喘、WBC、嗜中性粒细胞、补体C3及补体C4水平、抗SSA抗体阳性率并不是pSS患者发生ILD的影响因素。当pSS患者出现以上临床症状或实验室指标异常时,也应当警惕ILD的发生风险。
抗核抗体又称抗核酸抗原抗体,可特征性地出现于许多自身免疫性疾病中。高惠英等[19]研究发现, pSS-ILD患者与单纯pSS患者的抗核抗体阳性率比较无明显差异; 而王建军等[20]研究显示, pSS-ILD患者血清抗核抗体阳性率明显高于单纯pSS患者; 路武杰[21]研究发现, ILD是pSS常见的系统损害, pSS-ILD的发生与自身抗体有关; 国外研究[22]也证实, pSS-ILD的发生与抗核抗体存在密切关系。一项荟萃分析[23]显示,抗核抗体不是pSS-ILD发生的影响因素; 陈晓静等[9]研究表明,抗核抗体滴度升高(OR=0.585, 95%CI: 0.355~0.963, P=0.035)是非吸烟女性pSS患者出现ILD的独立危险因素; 蒋培培等[24]通过Logistic回归分析显示抗核抗体阳性率升高是pSS患者出现ILD的危险因素。而本研究通过多因素Logistic回归分析发现,高水平抗核抗体滴度是pSS患者发生ILD的独立危险因素,可能与样本量及纳入标准有关,还需深入研究。
综上所述,本组研究中pSS-ILD的发生率较高,高龄、吸烟及高抗核抗体滴度提示pSS患者发生ILD的风险明显增高。但本研究存在一定的局限性,部分临床资料无法获取,例如病理资料,且没有随访; 此外,ILD病理类型繁多,需要进行肺部组织活检,属于有创操作,在ILD的临床实践中并没有广泛普及。因此,今后还需要进一步深入分析。
-
![]()
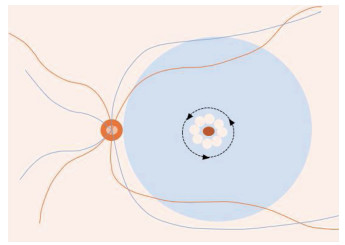
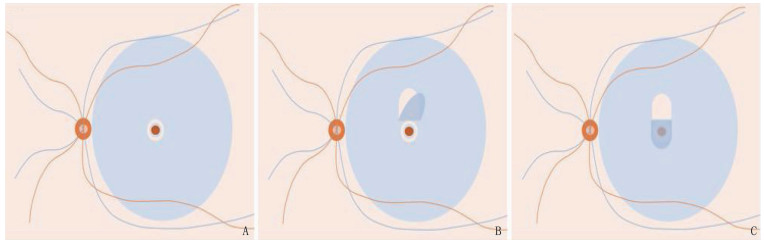
图 1 ILM剥离面积研究示意图
A: 视频终端实时显示以黄斑中心凹为中心的3个同心圆,直径分别1、2、3 PD; B: AIP小于3 PD; C: AIP大于3 PD。整体为ILM剥除术中眼底示意图,红色和蓝色曲线分别代表视网膜动静脉,左侧红色圆圈代表视盘,血管弓中间红色圆圈代表MH, 蓝色圆圈代表已染色的ILM, 蓝色圆圈中间的粉色区域代表剥除的ILM范围(本文所有示意图中均相同)。
![]()
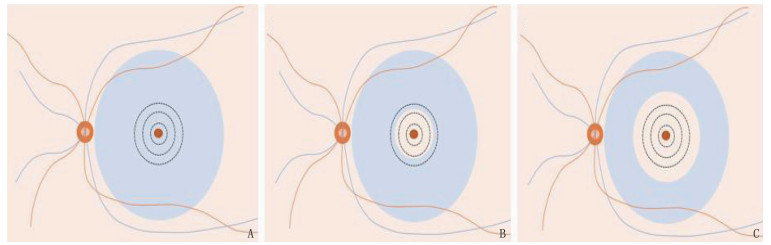
图 2 保留中心凹ILM剥离示意图
绕MH 1周分别重叠剥离数个圆形ILM, 保留MH边缘约500 μm的ILM。必要时可将ILM剥离区域扩展到孔周约2个PD范围(黑虚线)。
![]()
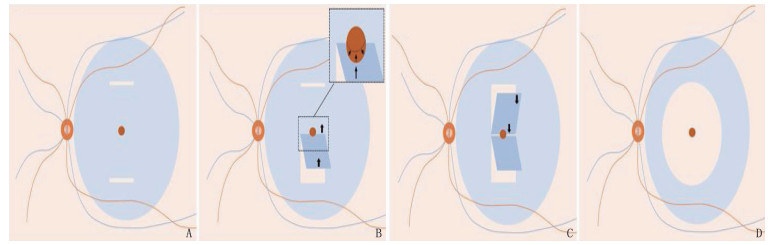
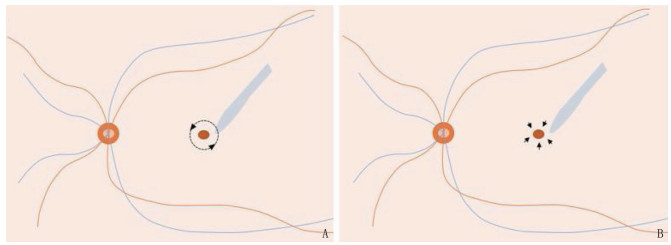
图 3 向心牵引ILM剥离示意图
A: 分别在裂孔上下象限近血管弓处剥离2条水平ILM带; B: 沿ILM带从下至上剥离下方矩形ILM瓣,向心性牵拉MH的下边缘; C: 以相同的方式从相反方向剥离上方的矩形ILM瓣牵拉MH的上边缘(B和C无先后顺序区分); D: 最后将MH周围进行圆形ILM剥除。
![]()
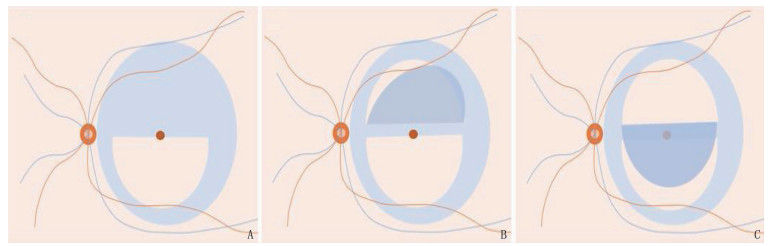
图 4 大型上半圆形ILM翻转覆盖术示意图
A: 先在下方血管弓至MH处完全剥除一个半圆形ILM; B: 在上方血管弓处不完全剥离一半圆形ILM瓣,剥离至距MH边缘100 μm处; C: 将半圆形ILM瓣翻转覆盖至MH上。
![]()
图 5 舌状ILM翻转覆盖术示意图
A: 先将MH周围的ILM环形剥离,宽度200~300 μm; B: 在MH上方视网膜不完全剥离制成舌状的ILM瓣; C: 再将舌状ILM瓣翻转覆盖在MH和无ILM的区域。
-
[1] GUYER D R, BUSTROS S D, DIENER-WEST M, et al. Observations on patients with idiopathic macular holes and cysts[J]. Arch Ophthalmol, 1992, 110(9): 1264-1268. doi: 10.1001/archopht.1992.01080210082030
[2] 孙天洋, 格日勒图. 黄斑裂孔研究进展[J]. 国际眼科杂志, 2021, 21(10): 1736-1740. doi: 10.3980/j.issn.1672-5123.2021.10.15 [3] LI Y T, JIN S Y, SHI L J, et al. Factors associated with anatomic failure and hole reopening after macular hole surgery[J]. J Ophthalmol, 2021, 2021: 7861180.
[4] LIN Y Y, LIU J H, CHANG Y. Foetal bovine serum can reduce toxicity of indocyanine green, brilliant blue G and trypan blue in ARPE-19 cellular model that suggests new surgical staining protocols for internal limiting membrane peeling procedure[J]. Clin Exp Ophthalmol, 2018, 46(7): 796-808. doi: 10.1111/ceo.13165
[5] WANG X W, LONG Y, GU Y S, et al. Outcomes of 4 surgical adjuvants used for internal limiting membrane peeling in macular hole surgery: a systematic review and network Meta-analysis[J]. Int J Ophthalmol, 2020, 13(3): 481-487. doi: 10.18240/ijo.2020.03.17
[6] LI S S, LI M, YOU R, et al. Efficacy of different doses of dye-assisted internal limiting membrane peeling in idiopathic macular hole: a systematic review and network meta-analysis[J]. Int Ophthalmol, 2021, 41(3): 1129-1140. doi: 10.1007/s10792-020-01656-2
[7] CARDOSO E B, MORAES-FILHO M, RODRIGUES E B, et al. Investigation of the retinal biocompatibility of acid violet for chromovitrectomy[J]. Albrecht Von Graefes Arch Fur Klinische Und Exp Ophthalmol, 2013, 251(4): 1115-1121. doi: 10.1007/s00417-013-2258-y
[8] PATONI POPESCU I S, MUŞAT O, STANCA S, et al. Vital dyes in macular hole surgery[J]. Exp Ther Med, 2021, 21(5): 527. doi: 10.3892/etm.2021.9959
[9] CHATZIRALLI I P, THEODOSSIADIS P G, STEEL D H W. Internal limiting membrane peeling in macular hole surgery; why, when, and how[J]. Retina, 2018, 38(5): 870-882. doi: 10.1097/IAE.0000000000001959
[10] DOGRAMACI M, WILLIAMSON T H. Dynamics of epiretinal membrane removal off the retinal surface: a computer simulation project[J]. Br J Ophthalmol, 2013, 97(9): 1202-1207. doi: 10.1136/bjophthalmol-2013-303598
[11] 黄惠嫔, 王艳菊, 柯瑞莉, 等. 两种内界膜剥离方式治疗MHCI < 0.7特发性黄斑裂孔的疗效[J]. 国际眼科杂志, 2019, 19(7): 1170-1173. [12] CAO J L, KAISER P K. Surgical management of recurrent and persistent macular holes: a practical approach[J]. Ophthalmol Ther, 2021, 10(4): 1137-1153. doi: 10.1007/s40123-021-00388-5
[13] BORAL S, DAS A, SINHA T. A novel standardized reproducible method to calculate the area of internal limiting membrane peeled intra-operatively in macular hole surgery by using a video overlay—a long-term study in cases of idiopathic macular holes[J]. Indian J Ophthalmol, 2020, 68(1): 157. doi: 10.4103/ijo.IJO_589_19
[14] NIE Z T, LIU B S, WANG Y, et al. Negative effects of enlarging internal limiting membrane peeling for idiopathic macular hole surgery[J]. Int J Ophthalmol, 2022, 15(11): 1806-1813. doi: 10.18240/ijo.2022.11.11
[15] HO T C, YANG C M, HUANG J S, et al. Foveola nonpeeling internal limiting membrane surgery to prevent inner retinal damages in early stage 2 idiopathic macula hole[J]. Albrecht Von Graefes Arch Fur Klinische Und Exp Ophthalmol, 2014, 252(10): 1553-1560. doi: 10.1007/s00417-014-2613-7
[16] MURPHY D C, FOSTIER W, REES J, et al. Foveal sparing internal limiting membrane peeling for idiopathic macular holes: effects on anatomical restoration of the fovea and visual function[J]. Retina, 2020, 40(11): 2127-2133. doi: 10.1097/IAE.0000000000002724
[17] GEENEN C, MURPHY D C, SANDINHA M T, et al. Significance of preoperative external limiting membrane height on visual prognosis in patients undergoing macular hole surgery[J]. Retina, 2019, 39(7): 1392-1398. doi: 10.1097/IAE.0000000000002137
[18] PENG J, ZHANG L H, CHEN C L, et al. Internal limiting membrane dragging and peeling: a modified technique for macular holes closure surgery[J]. Int J Ophthalmol, 2020, 13(5): 755-760. doi: 10.18240/ijo.2020.05.09
[19] SHUKLA D, KALLIATH J. Internal limiting membrane peeling for large macular hole: tailoring the rhexis to the shape of the hole[J]. Indian J Ophthalmol, 2022, 70(1): 182-186. doi: 10.4103/ijo.IJO_906_21
[20] JIANG T, ZHANG L M, WAN Q, et al. Comparative study of vitrectomy combined with internal limiting membrane peeling and vitrectomy combined with internal limiting membrane flap covering in idiopathic macular hole treatment: a meta-analysis and systematic review[J]. Ann Palliat Med, 2021, 10(5): 5474-5482. doi: 10.21037/apm-21-871
[21] MICHALEWSKA Z, MICHALEWSKI J, ADELMAN R A, et al. Inverted internal limiting membrane flap technique for large macular holes[J]. Ophthalmology, 2010, 117(10): 2018-2025. doi: 10.1016/j.ophtha.2010.02.011
[22] MICHALEWSKA Z, MICHALEWSKI J, DULCZEWSKA-CICHECKA K, et al. Temporal inverted internal limiting membrane flap technique versus classic inverted internal limiting membrane flap technique: a comparative study[J]. Retina, 2015, 35(9): 1844-1850. doi: 10.1097/IAE.0000000000000555
[23] CHEN S N. Large semicircular inverted internal limiting membrane flap in the treatment of macular hole in high myopia[J]. Graefes Arch Clin Exp Ophthalmol, 2017, 255(12): 2337-2345. doi: 10.1007/s00417-017-3808-5
[24] HU Z Z, QIAN H M, FRANSISCA S, et al. Minimal internal limiting membrane peeling with ILM flap technique for idiopathic macular holes: a preliminary study[J]. BMC Ophthalmol, 2020, 20(1): 228. doi: 10.1186/s12886-020-01505-x
[25] TAO M Y, WANG G Q, GOU Y Q, et al. Comparative study of conventional inverted ILM flap covering and ILM flap filling technique in idiopathic macular hole treatment: a meta-analysis and systematic review[J]. J Ophthalmol, 2022, 2022: 4922616.
[26] 赵培泉, 吕骄. 玻璃体切割手术治疗难治性黄斑裂孔的手术策略[J]. 中华眼底病杂志, 2020, 36(7): 495-498. doi: 10.3760/cma.j.cn511434-20200622-00301 [27] MAHAJAN V B, CHIN E K, TARANTOLA R M, et al. Macular hole closure with internal limiting membrane abrasion technique[J]. JAMA Ophthalmol, 2015, 133(6): 635-641. doi: 10.1001/jamaophthalmol.2015.204
[28] CAPOROSSI T, CARLÀM M, GAMBINI G, et al. Spotlight on the internal limiting membrane technique for macular holes: current perspectives[J]. Clin Ophthalmol, 2022, 16: 1069-1084. doi: 10.2147/OPTH.S284620
[29] TIBBETTS M D, REICHEL E, WITKIN A J. Vision loss after intravitreal ocriplasmin[J]. JAMA Ophthalmol, 2014, 132(4): 487. doi: 10.1001/jamaophthalmol.2013.8258
[30] JACKSON T L, HALLER J, BLOT K H, et al. Ocriplasmin for treatment of vitreomacular traction and macular hole: a systematic literature review and individual participant data meta-analysis of randomized, controlled, double-masked trials[J]. Surv Ophthalmol, 2022, 67(3): 697-711. doi: 10.1016/j.survophthal.2021.08.003
[31] LI J Q, BRINKEN R, HOLZ F G, et al. Silicone oil tamponade for persistent macular holes[J]. Eye, 2021, 35(8): 2206-2212. doi: 10.1038/s41433-020-01228-9
[32] LALLY D R, KASETTY M A. Closure of small macular holes using vitrectomy surgery with internal limiting membrane peeling without the use of intraocular gas tamponade: broadening the understanding of the macular hole pathophysiology[J]. RETINAL Cases Brief Rep, 2020, 14(2): 104-109. doi: 10.1097/ICB.0000000000000919
[33] YU Y P, LIANG X D, WANG Z Y, et al. Internal limiting membrane peeling and air tamponade for stage iii and stage iv idiopathic macular hole[J]. Retina, 2020, 40(1): 66-74. doi: 10.1097/IAE.0000000000002340
[34] 郁艳萍, 刘武. 重视特发性黄斑裂孔的临床研究[J]. 中华眼科医学杂志: 电子版, 2020, 10(3): 129-134. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHYB202003002.htm [35] WANG L F, WANG Y H, LI Y L, et al. Comparison of effectiveness between complete internal limiting membrane peeling and internal limiting membrane peeling with preservation of the central fovea in combination with 25G vitrectomy for the treatment of high myopic foveoschisis[J]. Medicine, 2019, 98(9): e14710. doi: 10.1097/MD.0000000000014710
[36] BURMEISTER S L, HARTWIG D, LIMB G A, et al. Effect of various platelet preparations on retinal muller cells[J]. Invest Ophthalmol Vis Sci, 2009, 50(10): 4881-4886. doi: 10.1167/iovs.08-3057
[37] HOERAUF H, KLÜTER H, JOACHIMMEYER E, et al. Results of vitrectomy and the no-touch-technique using autologous adjuvants in macular hole treatment[J]. Int Ophthalmol, 2001, 24(3): 151-159. doi: 10.1023/A:1021566806836
[38] ZHU D Q, MA B, ZHANG J, et al. Autologous blood clot covering instead of gas tamponade for macular holes[J]. Retina, 2020, 40(9): 1751-1756. doi: 10.1097/IAE.0000000000002651
[39] LI K R, ZHOU Y F, YANG W H, et al. Modified internal limiting membrane flap technique for large chronic macular hole: two case reports[J]. Medicine, 2022, 101(1): e28412. doi: 10.1097/MD.0000000000028412
[40] WANG H, JI M, DI R, et al. Parafoveal retinal massage combined with autologous blood cover in the management of giant, persistent or recurrent macular holes[J]. Int J Ophthalmol, 2020, 13(11): 1773-1779. doi: 10.18240/ijo.2020.11.14
[41] KUMAR A, TINWALA S I, GOGIA V, et al. Tapping of macular hole edges: the outcomes of a novel technique for large macular holes[J]. Asia Pac J Ophthalmol, 2013, 2(5): 305-309. doi: 10.1097/APO.0b013e31829a1919
[42] 王梦华, 姚佳, 李秋明. 内界膜剥除孔周按摩术与内界膜填塞术治疗较大孔径特发性黄斑裂孔的对比研究[J]. 眼科新进展, 2021, 41(11): 1062-1066. https://www.cnki.com.cn/Article/CJFDTOTAL-XKJZ202111013.htm [43] CHAKRABORTY D, SENGUPTA S, MUKHERJEE A, et al. Anatomical and functional outcomes one year after vitrectomy and retinal massage for large macular holes[J]. Indian J Ophthalmol, 2021, 69(4): 895-899. doi: 10.4103/ijo.IJO_1680_20
[44] MOHAMMED O A, PAI A. New surgical technique for management of recurrent macular hole[J]. Middle East Afr J Ophthalmol, 2017, 24(1): 61-63.
[45] STEEL D H, PARKES C, PAPASTAVROU V T, et al. Predicting macular hole closure with ocriplasmin based on spectral domain optical coherence tomography[J]. Eye, 2016, 30(5): 740-745. doi: 10.1038/eye.2016.42
 下载:
下载:
计量
- 文章访问数: 198
- HTML全文浏览量: 86
- PDF下载量: 32
 苏公网安备 32100302010246号
苏公网安备 32100302010246号
